Rectal Bleeding and Hemorrhoids: When It’s “Just Hemorrhoids” — and When It’s Not
Seeing blood in the toilet can be alarming—and it’s one of the most common reasons people search for hemorroid treatment. While
hemorrhoids are a frequent (and often benign) cause of rectal bleeding, not all bleeding is hemorrhoids. If you found this helpful, share it on social media so others know when to try conservative care and when to seek a medical evaluation.
Rectal Bleeding: Common Causes and Red Flags (hemorroid treatment + Colonoscopy)
Rectal bleeding simply means blood is coming from somewhere in the lower gastrointestinal (GI) tract—anywhere from the anus to the colon. The color and pattern can offer clues:
- Bright red blood on toilet paper or dripping into the bowl, often points to hemorrhoids or an anal fissure.
- Blood mixed in the stool, may suggest bleeding higher in the rectum or colon.
- Dark, maroon, or black stools, can indicate bleeding higher up in the GI tract and should be evaluated promptly.
Even if hemorrhoids are suspected, certain symptoms should raise concern and may warrant a **Colonoscopy** to rule out conditions like polyps, inflammatory bowel disease, diverticular bleeding, or colorectal cancer. Seek medical care promptly if you have:
- Persistent or heavy bleeding
- Dizziness, fainting, or shortness of breath (possible anemia)
- Unexplained weight loss
- New or worsening constipation/diarrhea
- Family history of colorectal cancer or polyps
- Bleeding starting at age 45+ (or earlier depending on risk)
The American College of Gastroenterology and other expert groups emphasize that rectal bleeding should not automatically be attributed to hemorrhoids—especially when accompanied by red-flag symptoms.
Hemorrhoids and Rectal Bleeding: What’s the Connection? (Hemorrhoid treatment)
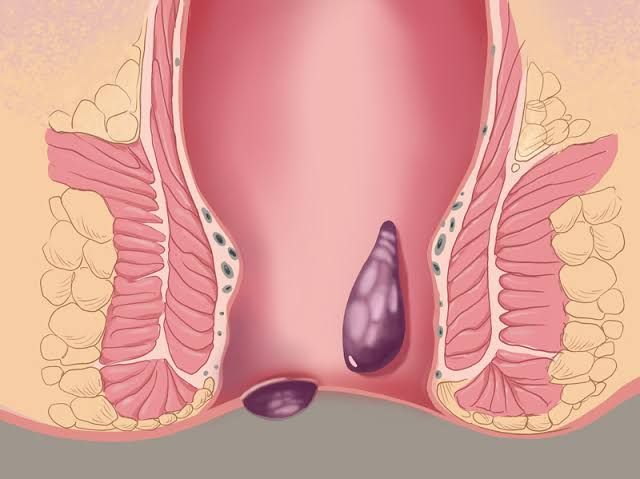
Hemorrhoids are swollen veins in the anal canal. They can be:
- Internal hemorrhoids, (inside the rectum): commonly cause painless bright red bleeding, sometimes with prolapse (bulging).
- External hemorrhoids, (under the skin around the anus): can cause pain, itching, and swelling; bleeding is less common unless irritated.
Typical hemorrhoid-related bleeding is small-volume, bright red, and may appear:
- on toilet paper,
- as streaks on stool,
- or as a few drops in the bowl.
Importantly, hemorrhoids can exist at the same time as other conditions. That’s why evaluation matters—especially if bleeding continues despite appropriate hemorroid treatment.
For an overview of hemorrhoid symptoms and care options, the National Institute of Diabetes and Digestive and Kidney Diseases provides patient-friendly guidance
Hemorroid Treatment Options: From Home Care to Office Procedures Most mild hemorrhoids improve with conservative measures.
Evidence-based first steps include:
1) Fiber + fluids
Increasing dietary fiber softens stool and reduces straining—one of
the biggest drivers of hemorrhoid bleeding. Options include high-fiber
foods and supplements (psyllium is commonly used).
2) Avoid straining and prolonged toilet sitting
Long bathroom sessions increase pressure in the hemorrhoidal veins.
3) Warm sitz baths
They can ease irritation and spasm.
4) Topical therapies
Short-term use of barrier creams or anti-itch preparations may help
symptoms, though they do not “cure” hemorrhoids.
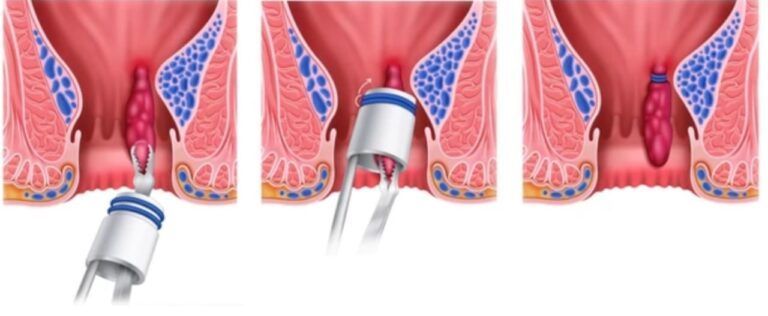
If bleeding persists or hemorrhoids prolapse, office-based treatments may be recommended. Rubber band ligation is commonly used for internal hemorrhoids and is supported as an effective outpatient option in many clinical reviews and society guidance [American Society of Colon and Rectal Surgeons—Hemorrhoids]
When a Colonoscopy Is Recommended for Rectal Bleeding
A Colonoscopy is not automatically required for every episode of bright red blood—especially in younger patients with classic hemorrhoid symptoms. However, it becomes more important when:
- bleeding is recurrent or unexplained,
- there are changes in bowel habits,
- stool tests suggest occult blood,
- anemia is present,
- or age/risk factors increase concern.
Colonoscopy is also central to colorectal cancer screening. The U.S. Preventive Services Task Force recommends routine screening beginning at age 45 for average-risk adults ([USPSTF—Colorectal Cancer.
- bleeding is recurrent or unexplained,
- there are changes in bowel habits,
- stool tests suggest occult blood,
- anemia is present,
- or age/risk factors increase concern.
Colonoscopy is also central to colorectal cancer screening. The U.S. Preventive Services Task Force recommends routine screening beginning at age 45 for average-risk adults.